
Obstructive Sleep Apnea
Introduction
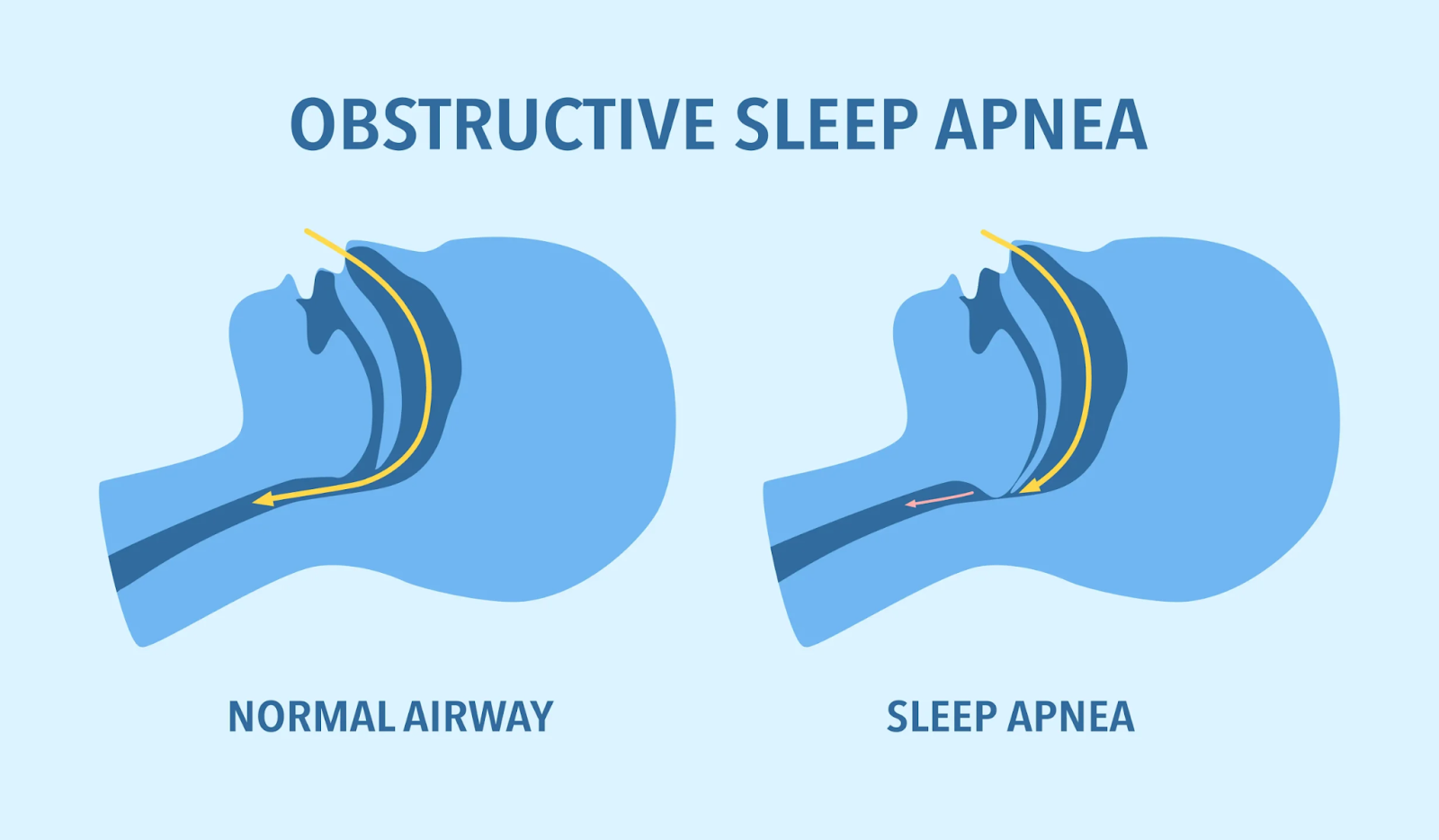
Apnea - complete collapse of upper airway.
Hypopnea - partial collapse of upper airway.
Obstructive sleep apnea (OSA) is a sleep disorder characterized by repeated episodes of apnea or hypopnea causing oxygen desaturation or sleep arousal. This leads to fragmented and non restorative sleep. It includes loud snoring, sudden awakening from sleep, excessive daytime sleepiness. OSA significantly affects cardiac health, behavioral conditions and quality of life.
Causes
OSA is a complex, multifactorial disorder. Sleep-related reductions in ventilatory drive, neuromuscular factors, and anatomical risk factors all contribute significantly to upper airway obstruction during sleep.
Anatomical factors:
An increase in pressure near the upper airway causes pharyngeal collapse (pharyngeal narrowing) leading to insufficient space for airflow in the upper airway during sleep. In addition, when the muscle tone in and around the neck is decreased, it may lead to partial or complete pharyngeal collapse.
Mandibular hypoplasia - decreased growth of jaw
Retrognathia - backward positioning of jaw
Micrognathia - small jaw
Adenoid or tonsillar hypertrophy
Inferior positioning of hyoid bone
Non anatomical factors
Male gender
Central fat distribution
Supine sleeping position
Pregnancy
Older age
Smoking
Alcoholism
Usage of sedative and hypnotic drugs
Associated medical conditions
Endocrine disorders like DM, metabolic syndrome, acromegaly, hypothyroidism
Neuro related disorders like stroke, myasthenia gravis, spinal cord injury
Prader Willi syndrome
Down’s syndrome
Congenital heart disease
Clinical features
Symptoms
Patients with OSA often experience excessive daytime sleepiness, loud disruptive snoring during sleep, gasping or choking during sleep (episodes of apnea), daytime fatigue.
Signs
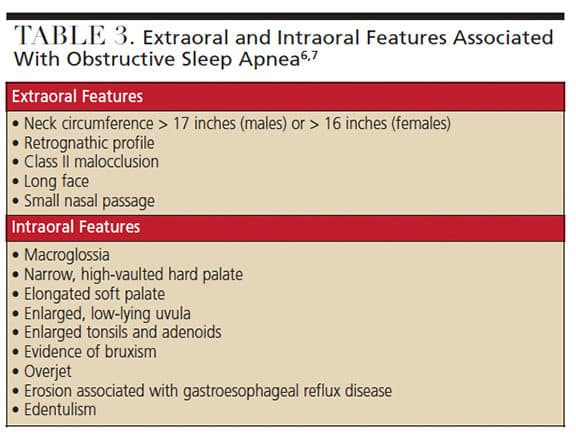
Obesity is one of the commonest findings in patients with OSA.
A large neck circumference (17 inches or 43 cm in males and 16 inches or 40.5 cm in females)
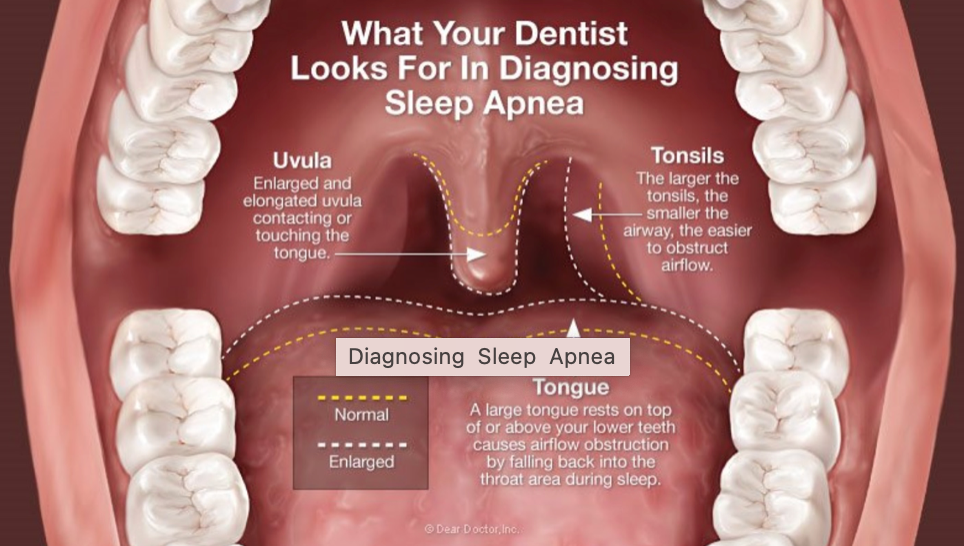
Crowded oropharynx
Retrognathia, micrognathia
Tonsillar hypertrophy
Low-lying palate
Overjet
Large tongue
Evaluation
Epworth Sleepiness Scale
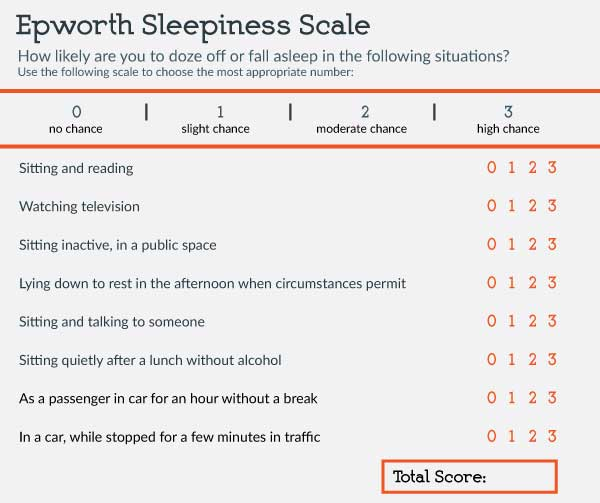
Epworth Sleepiness Score ranges from 0 to 24. A score above 9 suggests excessive daytime sleepiness.
STOP-BANG questionnaire
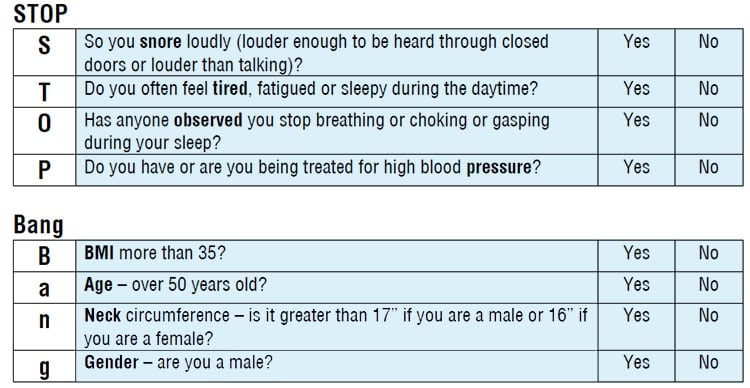
The STOP-BANG questionnaire can be used to assess the probability of moderate-to-severe OSA. A high risk is indicated if "YES" is selected for 5 or more items, while a low risk is indicated if "YES" is answered for fewer than 3 items.
Polysomnography
Night time laboratory level polysomnography is the gold standard test for evaluation of OSA. during the test, patients are monitored using electroencephalogram (EEG) leads, pulse oximetry, temperature and pressure sensors to detect nasal and oral airflow, respiratory impedance plethysmography belts around the chest and abdomen to monitor motion, an electrocardiogram (ECG) lead, and electromyogram sensors to detect muscle contractions in the chin, chest, and legs.
Scoring respiratory events in adults:
Oronasal thermal sensor
Nasal air pressure transducer
Inductance plethysmography (with esophageal manometry or a pressure catheter may be used as alternatives)
Pulse oximetry
Inference:
According to the American Academy of Sleep Medicine (AASM),
Hypopnea is defined by:
A reduction in airflow of at least 30% for more than 10 seconds, accompanied by at least 4% oxygen desaturation. (or)
A reduction in airflow of at least 30% for more than 10 seconds, associated with either at least 3% oxygen desaturation or an arousal from sleep on EEG.
Apnea is defined by:
A drop in the peak signal excursion by more than or equal to 90% of the pre-event baseline flow.
A duration of the flow reduction of more than or equal to 10 seconds.
Obstructive sleep apnea: If an increased effort is present throughout the entire apnea.
Central sleep apnea: If no effort is detected throughout the entire apnea.
Mixed apnea: Absence of effort during the initial portion of the event, followed by the resumption of effort in the latter part of the apnea.
Apnea - hypopnea index
The total number of apneas and hypopneas is divided by the total sleep time(hours) to get the events per hour.
Mild: 5 to 15 events per hour
Moderate: Greater than 15 to 30 events per hour
Severe: Greater than 30 events per hour
Complications
Hypertension
Myocardial infarction
Atrial fibrillation
Congestive heart failure
Cerebrovascular accident
Depression
Sleeplessness-related accidents
Management
Managing the OSA is a multidisciplinary approach.
Treating the underlying medical conditions
Lifestyle modifications - obesity management - weight loss, prioritizing 7 to 8 hours of night sleep, avoid alcohols, sedative - hypnotic drugs, smoking etc.
Positioning therapy: side position sleeping is advised
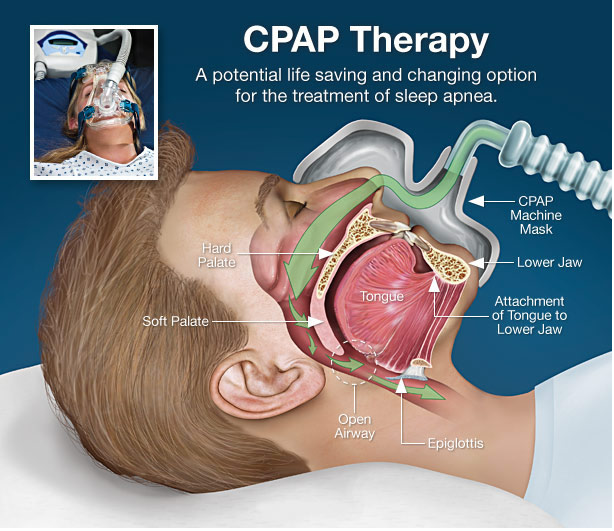
Continuous positive airway pressure therapy cPAP
It is most effective for adults. It involves using a machine to deliver mild air pressure through a mask, keeping the airways open during sleep. This prevents airway collapse and ensures uninterrupted breathing.
Oral appliance
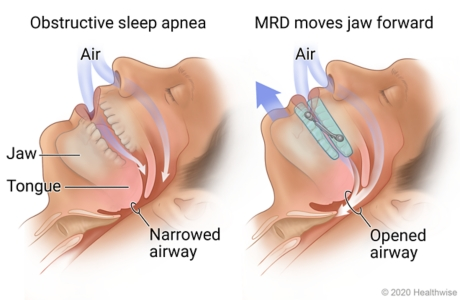
Mandibular advancement devices (MAD) can help alleviate airway obstruction by advancing the lower jaw.
This approach is typically most effective for candidates with appropriate dentition and mild-to-moderate sleep apnea.
The AASM and the American Academy of Dental Sleep Medicine (AADSM) have developed guidelines for using MAD in patients with OSA.
Oral appliances can be considered as an alternative to no treatment for adult patients with snoring (without OSA) or those with OSA who do not tolerate CPAP therapy or prefer an alternative treatment.
When a sleep physician prescribes oral appliance therapy for an adult patient with OSA, a qualified dentist should use a custom, titratable appliance.
A follow-up with a qualified dentist is necessary to assess for dental-related adverse effects after initiating oral appliance therapy in adult patients with OSA.
Follow-up sleep testing is required to confirm the efficacy of the treatment.
Surgical approaches
Tonsillectomy or adenoidectomy for their hypertrophy
Uvulopalatophrayngoplasty - surgical removal of the uvula and tissue from the soft palate to create more space in the oropharynx
Maxillomandibular advancement surgeries
Distraction osteogenesis for mandibular advancements in young patients
Hypoglossal nerve stimulation
In extreme cases, tracheostomy to bypass oropharyngeal obstruction
Conclusion
Managing OSA is most effectively achieved through an interprofessional team that includes a sleep specialist, dentist, cardiologist, otolaryngologist, dietitian, pulmonologist, neurologist, etc. Several treatment options are available for OSA, with the primary treatment being CPAP.
Adherence to CPAP use should be strongly encouraged, along with proper cleaning and maintenance of the machine to ensure optimal function.
Patients should also be educated on the importance of proper sleep hygiene, ensuring sufficient sleep each night, and the risks of driving while drowsy.
The short-term prognosis of OSA with treatment is generally favorable, but the long-term outlook remains uncertain.
The primary challenge is poor adherence to CPAP therapy, with nearly 50% of patients discontinuing its use within the first month despite education.
Many individuals with OSA have comorbidities or are at an increased risk for adverse cardiac events and stroke.
Consequently, individuals who do not adhere to CPAP are at a higher risk for cardiac and cerebral events, as well as increased annual healthcare-related costs.
Post a Comment